


Nothing obsesses our culture more than sex. Mating is not only a basic biological instinct, but an emotional one. References to, and discussions, surrounding sex and intimacy haunt every part of our culture. This ranges from the great works of romantic literature, to the commercial world of marketing.
It can be devastating when the penis does not work during an intimate moment. This can create confusion, concern, feelings of inadequacy and tension between partners. It need not be so; there are multiple avenues to consider when aiming to restore sexual function. This article aims to discuss the most important options.
Sex is like oxygen; it’s only a problem if you are not getting any.

Erectile dysfunction is a common disorder with up to 70% of men having an issue with it at some point in their life. The rate is naturally much higher for men above the age of 50, however surprisingly 5-10% of younger men report issues from time to time. In younger men, psychological issues are more common whilst in older men, underlying medical issues play more of a role.
How does an erection work?
A signal from the brain, or local touch to the penis, travels via the nerves to the penis. Here, the blood vessels relax and fill with blood. This blood occupies a space until full, which causes the penis to be erect.
What causes Erectile Dysfunction?

There are multiple factors towards erectile problems including:
1. Inflammation
- Inflammation describes the cell response when it is distressed
- This could be from a lack of nutrition, infection, too much sugar, insulin
- This also contributes to high oxidative stress; a form of chemical stress that damages cells
2. Endothelial dysfunction
- Endothelium refers to the cells that line our blood vessels
- The penis relies on blood flow to become erect
- Any issues such as blood vessel cell dysfunction, diabetes, cholesterol, high blood pressure or underlying medical issues will contribute to dysfunction here
3. Hormonal imbalance
- Healthy hormones are important for libido and sexual function
- Low testosterone is associated with erectile dysfunction
- Low progesterone can impact progesterone
4. Stress (Major factor)
- Emotional stress interrupts the nerve traffic that helps achieve a strong and normal erection
- The actual nerves supplying the penis can be damaged by diabetes, high cholesterol, smoking, alcohol and other medical conditions
- Sometimes, surgery of the prostate can damage the nerves going to the penis
5. Lack of sleep
- A lack of sleep is a major, underrecognised cause of erectile dysfunction
- Without good sleep, our brain cannot health overnight and create good hormones around the body

How is Erectile Dysfunction diagnosed?
A full history and review of a man’s health should be undertaken. All parts of health are important to achieve an erection.
One important question is how much of an erection the man is getting; is there a morning erection on waking up, can an erection start and then not sustain or is there nothing at all?
How does all this matter?
Erections that start strong but do not sustain are often psychogenic, that is caused by nerves or anxiety. This is even more the case if the man is young, can masturbate with a full erection and wakes with ‘morning glory’ aka morning erection.
Mild erectile dysfunction typically involves an erection being achieved, but not sustained to the point of dual orgasm; ‘half mast.
Finally, if a man has no morning erections and cannot begin one prior to sexual activity, underlying medical issues should be explored.

Premature ejaculation ( PE )
Premature ejaculation is the elephant in the room. PE is a separate problem to erectile dysfunction, however rates of PE are substantially higher in men with erection issues. PE is often due to a changed nature of the nervous feedback from the penis; without a full erection, the sensation is different. Similarly, problems with nerves that may lead to PE can also cause erectile dysfunction. Premature ejaculation and erectile dysfunction should be treated together.
Top Tip: Premature ejaculation can be treated with graded masturbation exercises as well as a class of medication called Selective Serotonin Reuptake Inhibitors. Viagra/Cialis are useful. The patient should speak to their doctor about options.
What are the treatment options for Erectile Dysfunction?
Treatment should take into consideration any underlying medical issues working against the erection. The body is a whole and what is good for the body is good for the penis.
- Fix any underlying nutritional or vitamin deficiencies.
- Balance any hormones; replace testosterone if needed.
- Improve endothelial function: L arginine, antioxidants, nitrous releasing compounds.
- Weight loss, exercise and cutting alcohol and smoking are not negotiable!
- PDE5 inhibitors such as viagra, stendra or cialis.
- Address any prostate issues; prostatic enlargement will impede erections.
- Psychological support and relationship support; erections mostly start in the mind.
- Address any medications that may cause erectile dysfunction like ‘beta blockers’.
Top Tip: If a man has an enlarged prostate, begin treatment with tamsulosin. This class of medication relaxes the smooth muscle of the prostate but has a net positive impact on erections. Another class of prostate medication is 5 alpha reductase blocker; these lower the amount of testosterone causing the prostate to grow. They are effective, however can work against erections in some men.
What about medications for erectile dysfunction?
Once the underlying medical issues have been addressed, the first line of treatment for erectile dysfunction is something called a PDE5 inhibitor. Popular names in this category include Viagra, Cialis and stendra. These medications work by relaxing the blood vessels in the penis and prolonging the erect phase.
Treatment Tips:
Cialis has a longer half life (18 hours) than Viagra.
5mg per day reduces prostatic tension and also generally treats mild erectile dysfunction cases.
An additional 20mg of cialis or a viagra can be taken on top of this for more difficult cases.
Stendra is not superior to Viagra; it just has less side effects.
Cialis and Viagra are the first line treatments. Cialis is taken at 5mg per day, or 20mg before sexual activity. Viagra is taken at 50-100mg half an hour before sexual activity. Side effects include blue vision and the medication should be avoided if there has been a recent heart attack.
If an erection lasts longer than 4 hours, the patient should seek emergency care.
What are the risks of Viagra or Cialis?
Viagra and Cialis are generally safe.
They should not be used within 3 months of a heart attack or illness In a small number of men, it may cause blue vision.
If there are any palpitations or feeling tightness of breathing, stop sexual activity and phone an ambulance immediately.
Take half a tablet half an hour before sexual activity.
If an erection lasts longer than 5 hours, head to hospital without delay. I have reviewed other medications prior to prescribing.
What is a Vacuum Erectile Device?
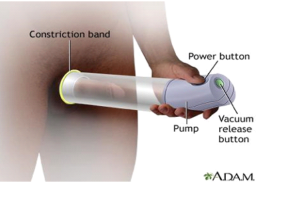
Immortalised in the Austin Powers movies as the ‘Swedish Penis Pump’, the vacuum erectile device has seen action for decades. The pump uses a vacuum to open the blood filled chambers of the penis, called the corporal sinusoids. By opening up these chambers, the device induces an erection.
The VED was traditionally used to induce an erection. In patients who have had their nerves damaged in prostate surgery, the VED has been used in ‘penile rehabilitation’ therapy. This involves the use of the VED for ten minutes, alongside Viagra, three times per week. Studies showed a 60% improvement in erections and 80% satisfaction rate.
Interestingly, the VED was largely successful in preventing the shortening of the penis in prostate surgery patients. However, studies have not shown any elongation of the penis in any other group from using the VED.
Given that a VED is low risk, non-medication based and affordable, it is a reasonable second line treatment after Cialis/Viagra alone for any man not responding to those treatments.
What is a penile ring?
Reference: https://www.hims.com/sexual-health/penis-rings
A penile ring is a constrictive device which blocks outflow of blood from the corporal sinusoids. Colloquially, it is known as a cock ring. There is very little evidence on the efficacy of a penile ring. The ring should not be worn for more than 30 minutes, be one that is easily removed, not be made of metal and the use should follow careful reading of the instructions.
Shockwave Therapy
Low intensity extracorporeal shockwave therapy describes a novel technology to treat erectile dysfunction. The theory is that high energy sound waves can speed up tissue repair and cell growth and improve erection function.
Shockwave therapy is currently controversial; many of the scientific studies are suboptimal and there is a difference between the weaker, potentially ineffective Class 1 devices being used in the market versus the Class 2 more powerful devices that have largely been used in trials.
The process involves shockwave therapy being administered at several points along the penis over a session, such as 15 minutes, typically twice weekly for 3 weeks. This is repeated for another 3 weeks after a 3 week break. The studies are promising, however much more research is needed before this technique can be soundly recommended.
Penis injections
Intracorporeal or intracavernosal injections involve a medication being injected directly into the blood chambers of the penis. The success rate is about 50%, however the discontinuation rate is very high. Intracorporeal injections remain an important treatment for men with erectile dysfunction. However, understandably, they are often reserved for very serious cases where simpler options have been exhausted.
Penile Filler
It is not a surprise that very soon after the popularisation of cosmetic filler, used to give volume in the face, that some of it found its way into a penis. Used to increase the ‘girth’ of the penis, the penile filler procedure does not address the erection issue per se. It might be an adjunct if there is a partial erectile dysfunction to add size in the context of ‘half a mongrel’.
Future and alternative treatments
The future of erectile dysfunction involves stem cells, growth factor injections and other novel treatments. Currently, Platelet Rich Plasma is being investigated; however studies are small and this is not currently recommended.
Another treatment option is penile prostheses; this is best discussed with a consultant Urologist who is a specialist in this line of treatment.
You can read about relevant health topics by clicking the articles below:
- Oxidative Stress
- Inflammation
- Sleep and the brain
- Testorone
REFERENCES
Belew D, Klaassen Z, Lewis RW. Intracavernosal Injection for the Diagnosis, Evaluation, and Treatment of Erectile Dysfunction: A Review. Sex Med Rev. 2015;3(1):11-23. doi:10.1002/smrj.35
Dong L, Chang D, Zhang X, et al. Effect of Low-Intensity Extracorporeal Shock Wave on the Treatment of Erectile Dysfunction: A Systematic Review and Meta-Analysis. Am J Mens Health. 2019;13(2):1557988319846749.
doi:10.1177/1557988319846749
Duncan C, Omran GJ, Teh J, Davis NF, Bolton DM, Lawrentschuk N. Erectile dysfunction: a global review of intracavernosal injectables. World J Urol. 2019;37(6):1007-1014. doi:10.1007/s00345-019-02727-5
Epifanova MV, Gvasalia BR, Durashov MA, Artemenko SA. Platelet-Rich Plasma Therapy for Male Sexual Dysfunction: Myth or Reality?. Sex Med Rev. 2020;8(1):106-113. doi:10.1016/j.sxmr.2019.02.002
Gruenwald I, Appel B, Vardi Y. Low-intensity extracorporeal shock wave therapy–a novel effective treatment for erectile dysfunction in severe ED patients who respond poorly to PDE5 inhibitor therapy. J Sex Med. 2012;9(1):259-264. doi:10.1111/j.1743- 6109.2011.02498.x
Hoyland K, Vasdev N, Adshead J. The use of vacuum erection devices in erectile dysfunction after radical prostatectomy. Rev Urol. 2013;15(2):67-71.
Huang YC, Wu CT, Chen MF, Kuo YH, Li JM, Shi CS. Intracavernous Injection of Autologous Platelet-Rich Plasma Ameliorates Hyperlipidemia-Associated Erectile Dysfunction in a Rat Model. Sex Med. 2021;9(2):100317.
doi:10.1016/j.esxm.2020.100317
Lin H, Wang R. The science of vacuum erectile device in penile rehabilitation after radical prostatectomy. Transl Androl Urol. 2013;2(1):61-66. doi:10.3978/j.issn.2223- 4683.2013.01.04
Poulios E, Mykoniatis I, Pyrgidis N, et al. Platelet-Rich Plasma (PRP) Improves Erectile Function: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. J Sex Med. 2021;18(5):926-935. doi:10.1016/j.jsxm.2021.03.008

